
If you thought you left acne behind in high school, only to find yourself dealing with painful breakouts in your 40s or 50s, you’re definitely not alone. Menopausal acne affects somewhere between 40-55% of women during perimenopause and menopause—and if you’re searching for menopausal acne pictures, you’re probably trying to figure out if what you’re experiencing is normal.
Here’s the short answer: yes, it’s normal, and yes, there are real solutions that work.
This isn’t your teenage acne making a comeback. Menopausal acne looks different, behaves differently, and requires different treatment approaches. In this guide, we’ll walk through what menopausal acne actually looks like, why it happens, where it typically shows up, and most importantly—how to treat it effectively.
What Does Menopausal Acne Look Like? Visual Characteristics
While everyone’s skin is different, menopausal acne has some distinctive characteristics that set it apart from the breakouts you might remember from your teenage years.
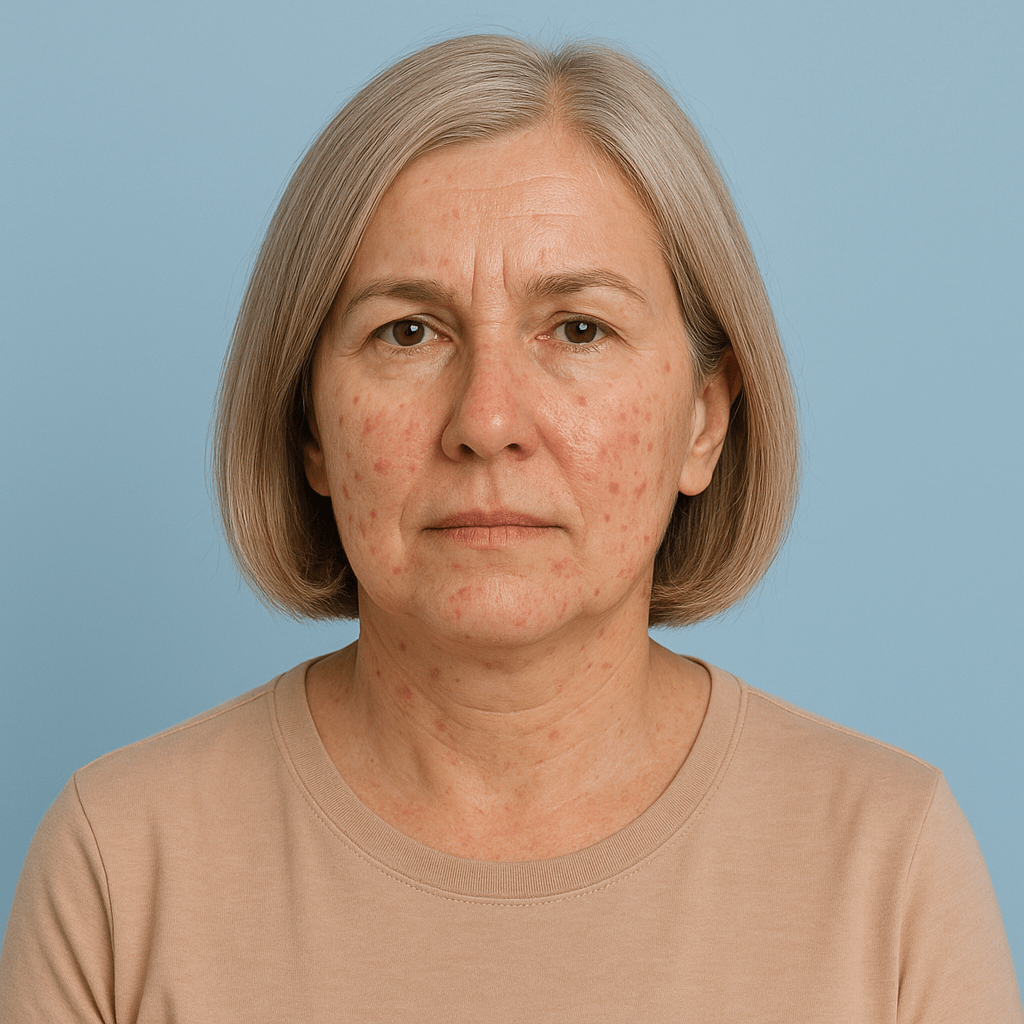
Overall Appearance: Menopausal acne tends to present as deeper, more inflamed lesions that are slower to heal. Rather than the mix of blackheads, whiteheads, and surface pimples common in adolescence, menopausal acne typically appears as red to purple, under-the-skin inflammation that feels painful to the touch.
Color and Texture: Active menopausal breakouts often show up as deep red or even purplish bumps beneath the skin’s surface. Unlike surface pimples with visible white or yellow heads, these lesions remain under the skin, creating hard, tender lumps that can persist for weeks. When they do eventually surface, they’re often larger and more inflamed than typical teenage acne.
Size and Depth: These breakouts are usually larger—think dime-sized or bigger—and you can feel them well before you see them. They start as tender areas under the skin and gradually develop into visible, raised bumps.
Healing Patterns: One of the most frustrating aspects of menopausal acne is how long it takes to heal. Where a teenage pimple might clear up in 3-7 days, menopausal acne can linger for 2-4 weeks or even longer. The deeper inflammation also means a higher risk of scarring and post-inflammatory hyperpigmentation (those dark marks that remain long after the breakout heals).
According to the American Academy of Dermatology, adult acne is becoming increasingly common, with unique characteristics that require specialized treatment approaches.
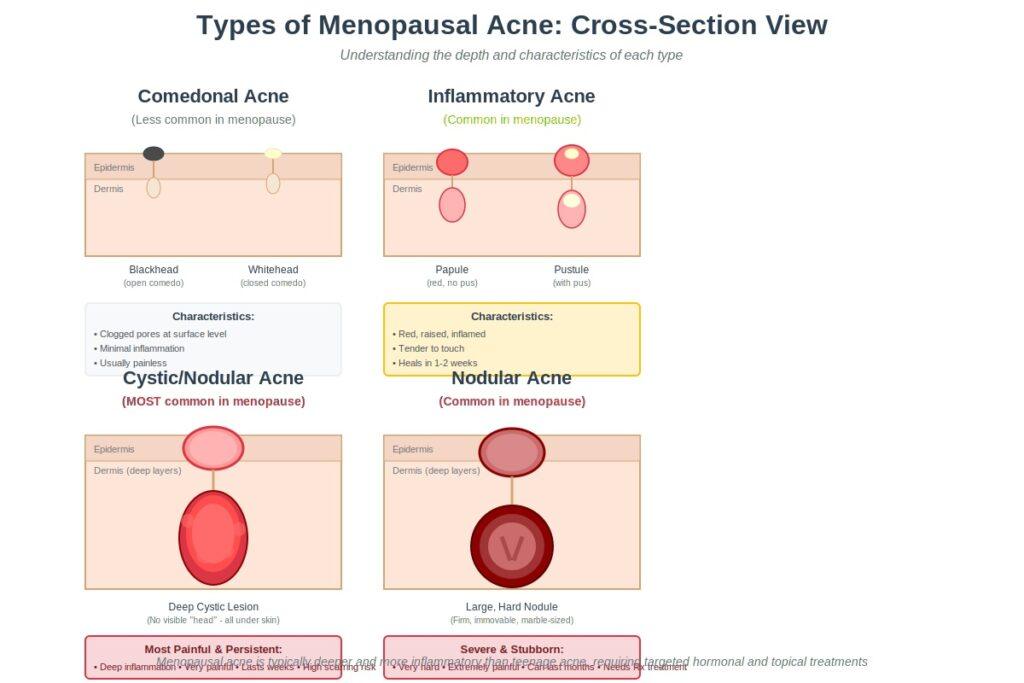
Types of Menopausal Acne
Understanding what type of acne you’re dealing with helps you choose the right treatment approach.
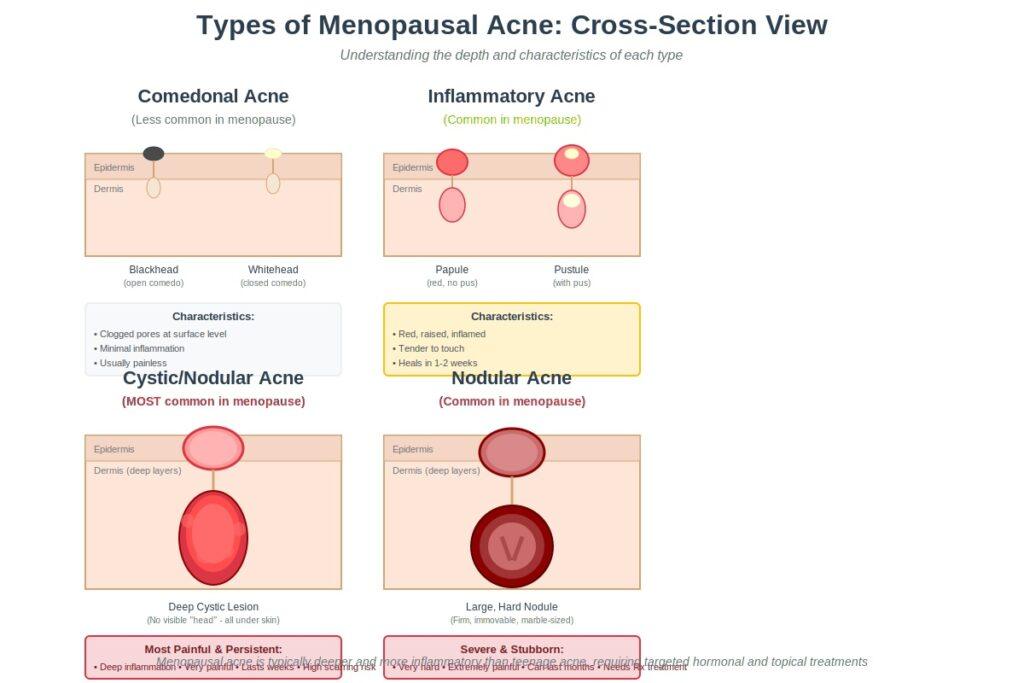
Inflammatory Acne (Papules and Pustules)
These are red, inflamed bumps that may or may not have a visible white head. Papules are the solid, raised bumps without pus, while pustules have that characteristic white or yellow center. During menopause, these tend to be larger and more tender than their teenage counterparts.
Common locations: Jawline, chin, around the mouth
Duration: 1-2 weeks typically
Pain level: Moderate to significant, especially when touched
Cystic Acne
This is the most common—and most frustrating—type of menopausal acne. Cystic acne consists of deep, painful lumps under the skin that never develop a “head” you can see. These lesions form deep in the skin’s layers and can feel like hard, immovable bumps.
Why hormonal changes trigger this type: As estrogen levels decline during menopause, the relative dominance of androgens (even at normal levels) triggers increased sebum production and inflammation deep within hair follicles. This creates the perfect environment for cystic lesions.
Common locations: Lower face, especially jawline and chin
Duration: Can persist for weeks or even months
Pain level: Often quite painful, especially when the area is touched
Scarring risk: High—these deep lesions can leave lasting scars
Nodular Acne
Similar to cystic acne but even larger and harder, nodular acne creates firm bumps deep under the skin. These can be as large as a marble and are often resistant to typical acne treatments.
Common locations: Jawline, chin, and sometimes neck
Duration: Weeks to months without treatment
Treatment challenges: Often requires prescription medication or in-office procedures
Comedonal Acne (Blackheads and Whiteheads)
While less common as the primary type during menopause, some women do experience blackheads and whiteheads alongside deeper breakouts. These are caused by clogged pores and are linked to the changing skin texture that occurs during menopause as skin becomes thinner and collagen production slows.
Common locations: Can appear anywhere but less predictable than inflammatory acne
Duration: Can persist until extracted or treated
Pain level: Usually minimal unless they become inflamed
Where Menopausal Acne Typically Appears
One of the telltale signs that your acne is hormonal in nature is where it shows up.
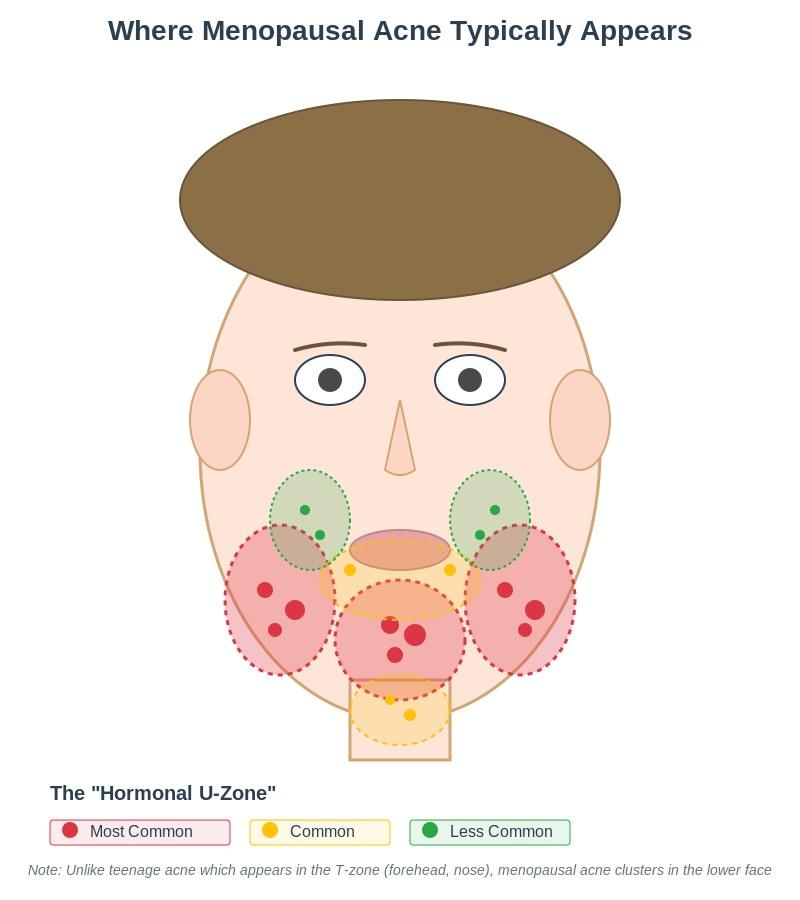
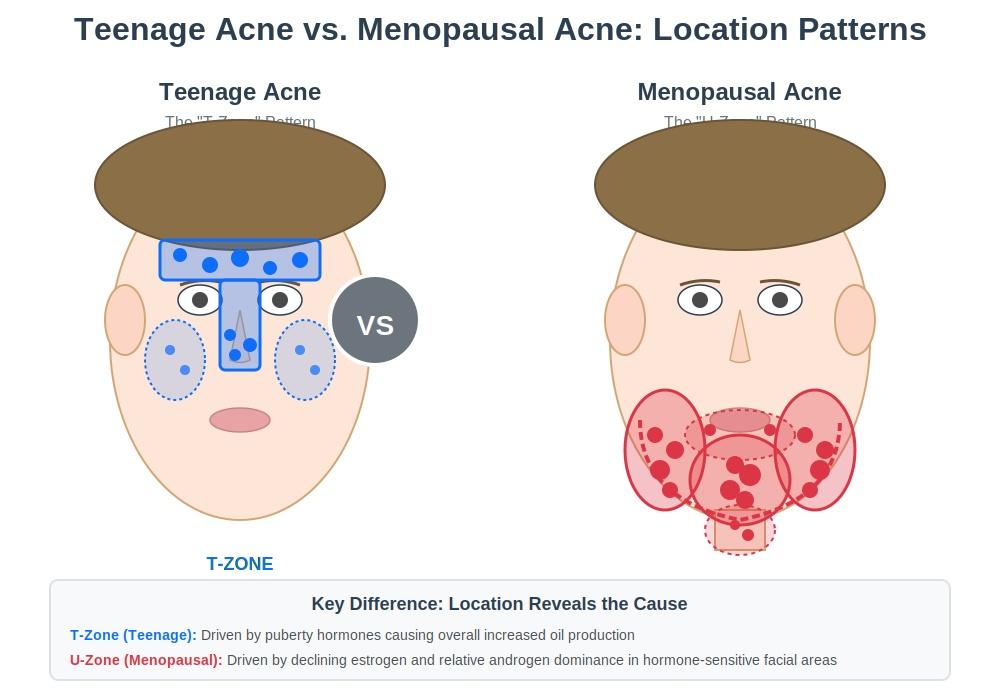
The Hormonal Zone: Lower Face Pattern
Menopausal acne has a distinctive distribution pattern, clustering primarily on the lower third of the face:
Jawline: This is ground zero for hormonal acne. The jawline and jaw angles are the most common areas for menopausal breakouts, often in a pattern that follows the jaw’s shape.
Chin: The chin and area around the chin are second most common, with breakouts often appearing in clusters or as single, large cystic lesions.
Around the Mouth: The area surrounding the mouth, including just below the lower lip and at the corners, frequently develops hormonal acne during menopause.
Neck: Yes, neck acne is absolutely a thing during menopause. Breakouts can extend down from the jawline onto the upper neck, which can be particularly uncomfortable.
Other Common Areas
Cheeks: While less common than lower face breakouts, some women do experience acne on their cheeks during menopause, particularly the lower cheek area near the jawline.
Chest and Back: In more severe cases, menopausal acne can extend to the chest, shoulders, and back. This is less common but tends to occur in women with more significant hormonal imbalances.
This lower face pattern is what dermatologists call the “hormone belt” or “U-zone.” According to research published in the Journal of Clinical and Aesthetic Dermatology, this distribution pattern is a key diagnostic feature of hormonal acne and differs significantly from teenage acne, which typically concentrates in the “T-zone” (forehead, nose, and cheeks).
Why Menopause Causes Acne: The Hormonal Science
Understanding why this is happening can help you feel less frustrated and more empowered to find solutions.
The Estrogen-Androgen Shift
During your reproductive years, estrogen helps regulate sebum (oil) production and keeps androgens in check. As you enter perimenopause and menopause, estrogen levels decline significantly—sometimes by as much as 60-80%.
Here’s where it gets interesting: even if your testosterone and other androgen levels stay exactly the same, the ratio changes. With less estrogen in the picture, androgens have a relatively stronger effect on your skin. This is called “relative androgen dominance,” and it’s the primary driver of menopausal acne.
These androgens bind to receptors in your skin’s sebaceous glands, triggering:
- Increased sebum production
- Thicker sebum that more easily clogs pores
- Increased inflammation in hair follicles
- Slower skin cell turnover
The North American Menopause Society notes that these hormonal shifts affect virtually every system in the body, with skin changes being among the most visible.
The Timeline of Hormonal Changes
Perimenopause (typically 40s): This is often when acne starts or returns. Your estrogen levels are fluctuating wildly—high one month, low the next—which can trigger unpredictable breakouts.
Early Menopause: Acne often peaks during the first few years after your final period, when estrogen levels have dropped significantly but haven’t yet stabilized.
Post-Menopause (5+ years after final period): Most women see improvement during this phase as hormone levels stabilize at their new, lower baseline. However, some women continue to experience occasional breakouts.
Individual Variation: Some women never get menopausal acne, while others struggle for years. Genetics, stress levels, other hormonal conditions, and skincare habits all play a role.
Other Contributing Factors
Stress and Cortisol: Let’s be honest—menopause is stressful. Hot flashes, sleep disruption, mood changes, and life stress during your 40s and 50s all contribute to elevated cortisol, which can worsen acne.
Insulin Resistance: Many women develop increased insulin resistance during menopause, which can contribute to both weight gain and acne. Insulin stimulates androgen production, creating a cycle that promotes breakouts.
Declining Skin Barrier Function: As estrogen drops, your skin’s barrier function weakens, collagen production slows, and skin becomes thinner. This makes your skin both more prone to irritation and less able to recover from breakouts.
Menopausal Acne vs. Teenage Acne: Key Differences
This isn’t the same acne you dealt with (or didn’t deal with) as a teenager. Here’s how they differ:
| Characteristic | Teenage Acne | Menopausal Acne |
|---|---|---|
| Primary Location | Forehead, nose, cheeks (T-zone) | Jawline, chin, lower face (U-zone) |
| Type | Mix of blackheads, whiteheads, papules, pustules | Primarily deep, cystic, inflammatory lesions |
| Healing Time | 3-7 days typically | 2-4 weeks or longer |
| Underlying Cause | Puberty hormones, increased overall oil | Declining estrogen, relative androgen dominance |
| Skin Type | Often oily all over | Often dry with localized breakouts (confusing!) |
| Scarring Risk | Moderate | Higher due to deeper inflammation |
| Treatment Response | Generally quick | Slower, requires more patience |
| Skin Texture | Young, resilient | Mature, thinner, more sensitive |
One of the most frustrating aspects of menopausal acne is dealing with what seems like contradictory skin conditions: you’re breaking out and developing fine lines, you need acne treatment and anti-aging products, your skin is dry and oily. This combination requires a nuanced approach that addresses both concerns without making either worse.
The treatments that worked when you were 16 probably won’t work now—and might actually make things worse. Your mature skin can’t tolerate the harsh, drying treatments that teenage skin can handle.
Identifying Your Menopausal Acne: Self-Assessment Guide
You likely have menopausal acne if you:
- ✓ Are in your 40s-60s (perimenopause, menopause, or early post-menopause age)
- ✓ Experience breakouts primarily on your lower face, jawline, and chin
- ✓ Notice deep, painful bumps rather than surface pimples
- ✓ Have breakouts that last weeks rather than days
- ✓ Didn’t have significant acne as a teenager, or your current acne is very different from what you experienced then
- ✓ Notice correlation with menstrual cycle changes (if you’re still cycling irregularly)
- ✓ Have other menopause symptoms like hot flashes, night sweats, irregular periods, mood changes, or sleep disruption
- ✓ Find your skin is both dry AND breaking out simultaneously
- ✓ Notice the acne gets worse with stress
When It Might Be Something Else
While menopausal acne is common, sudden, severe acne accompanied by other symptoms could indicate a different hormonal condition that requires medical evaluation:
- Sudden onset of severe acne with no previous history
- Excessive facial hair growth (hirsutism)
- Rapid, unexplained weight gain
- Thinning scalp hair while body hair increases
- Severe fatigue beyond typical menopause symptoms
These could indicate conditions like polycystic ovary syndrome (PCOS), thyroid disorders, or adrenal issues. According to the Mayo Clinic, adult acne that appears suddenly or is accompanied by other symptoms warrants a medical evaluation.
Treatment Options for Menopausal Acne
The good news: multiple effective treatments exist. The better news: you don’t have to just live with this.
Hormone Replacement Therapy (HRT) and Acne
For many women, addressing the root hormonal cause provides the most effective long-term solution.
How HRT Helps: By restoring estrogen levels, HRT can rebalance the estrogen-androgen ratio that’s causing your breakouts. Estrogen helps regulate sebum production, reduces inflammation, and improves skin barrier function.
Timeline for Improvement: Don’t expect overnight results. It typically takes 3-6 months of consistent HRT use to see significant improvement in acne. Your skin needs time to respond to the hormonal changes.
Types of HRT: Estrogen therapy (with or without progesterone) can help, but the type of progestin matters significantly. Some progestins have androgenic properties that can actually worsen acne, while others have anti-androgenic effects that help.
Best progestins for acne:
- Drospirenone (found in some HRT formulations)
- Micronized progesterone (generally neutral to slightly helpful)
Progestins that may worsen acne:
- Norethindrone
- Levonorgestrel
- Medroxyprogesterone acetate
Important Considerations: HRT isn’t right for everyone. Women with a history of certain cancers, blood clots, or other conditions may not be candidates. The decision to use HRT should be made with your healthcare provider, considering your overall health profile and menopause symptoms beyond just acne.
The North American Menopause Society provides comprehensive information about HRT benefits and risks.
Topical Treatments
Topical treatments work on the skin’s surface to unclog pores, reduce inflammation, and prevent new breakouts.
Retinoids (Prescription and OTC):
Retinoids are the gold standard for both acne and anti-aging, making them perfect for menopausal acne. They increase cell turnover, unclog pores, reduce inflammation, and boost collagen production.
- Prescription options: Tretinoin (Retin-A), adapalene (Differin—now also OTC), tazarotene
- OTC options: Retinol, adapalene 0.1%
How to use: Start low and go slow. Mature skin is more sensitive than teenage skin. Begin with 2-3 times per week and gradually increase frequency. Apply to clean, dry skin, wait 20-30 minutes, then moisturize.
Expected timeline: You may experience a “purging” period (increased breakouts) during weeks 2-6 as the retinoid brings existing clogs to the surface. Real improvement typically shows up around the 8-12 week mark.
Critical: Use sunscreen daily. Retinoids increase sun sensitivity, and sun damage is cumulative.
Benzoyl Peroxide:
This antibacterial ingredient kills acne-causing bacteria and helps unclog pores. However, it can be drying and irritating, especially on mature skin.
Best practices for mature skin:
- Use lower concentrations (2.5-5% rather than 10%)
- Apply as a spot treatment rather than all over
- Use only in the evening to avoid interactions with other products
- Moisturize well
Salicylic Acid:
This beta hydroxy acid (BHA) penetrates into pores to dissolve the oil and dead skin cells that cause clogs. It’s gentler than benzoyl peroxide and works well for mature skin.
Recommended concentration: 0.5-2% for daily use
How to use: Look for cleansers, toners, or leave-on treatments
Bonus benefit: Helps with texture and fine lines
Azelaic Acid:
This multi-tasker is anti-inflammatory, antibacterial, and helps fade post-inflammatory hyperpigmentation—those dark marks left behind after breakouts heal.
Why it’s great for menopausal skin: It’s well-tolerated by sensitive, mature skin and addresses both acne and aging concerns.
Available as: 10% OTC or 15-20% prescription
Can be used: Morning or evening, works well with other actives
Niacinamide:
Vitamin B3 (niacinamide) regulates sebum production, reduces inflammation, strengthens the skin barrier, and improves texture and tone.
Recommended concentration: 5-10%
Why it works for menopause: Addresses multiple skin concerns simultaneously without irritation
Compatibility: Can be layered with almost any other active ingredient
The American Academy of Dermatology provides evidence-based guidance on topical acne treatments.
Oral Medications
When topical treatments aren’t enough, oral medications that address hormonal causes from the inside can be game-changers.
Spironolactone:
This is the gold standard oral medication for hormonal acne in women. Originally developed as a blood pressure medication and diuretic, it has anti-androgen properties that make it incredibly effective for hormonal acne.
How it works: Spironolactone blocks androgen receptors in the skin, preventing testosterone and other androgens from triggering oil production and inflammation.
Typical dosing: 50-200mg daily (most women respond well to 100mg)
Timeline for results: 3-6 months for full effect
Important note: Requires ongoing use—acne typically returns if you stop
Side effects: Breast tenderness, irregular periods (if still cycling), increased urination initially, possible potassium elevation (requires monitoring)
Who shouldn’t use it: Women with kidney problems, high potassium levels, or who are pregnant
According to Cleveland Clinic, spironolactone is highly effective for hormonal acne with a good safety profile for long-term use.
Oral Contraceptives:
For perimenopausal women who are still having periods (even irregular ones), birth control pills with anti-androgenic progestins can help both regulate cycles and clear acne.
Best options for acne:
- Pills containing drospirenone (Yaz, Yasmin)
- Pills with cyproterone acetate (not available in US)
Benefits: Birth control + acne treatment + can ease perimenopause symptoms
Considerations: Not appropriate for women over 35 who smoke or have certain health conditions
Antibiotics:
Oral antibiotics like doxycycline and minocycline reduce inflammation and kill acne-causing bacteria.
Important limitations:
- Should only be used short-term (3-6 months maximum)
- Not a long-term solution
- Antibiotic resistance is a growing concern
- Often used as a bridge while waiting for other treatments to work
Isotretinoin (Accutane):
For severe, resistant menopausal acne, isotretinoin can be highly effective. This powerful medication essentially “resets” your oil glands.
Considerations for mature skin:
- Side effects (severe dryness, sensitivity) can be more impactful on aging skin
- Requires careful monitoring and pregnancy prevention
- Usually reserved for cases that haven’t responded to other treatments
- Can provide lasting or even permanent improvement
Skincare Routine for Menopausal Acne-Prone Skin
The challenge with menopausal acne is that you need to treat acne while also caring for mature, often drier skin. Here’s how to do both.
Morning Routine
1. Gentle Cleanser
Skip harsh, stripping cleansers. Look for pH-balanced, non-foaming or light-foaming cleansers that clean without destroying your skin barrier.
What to look for: Glycerin, ceramides, gentle surfactants
What to avoid: Sodium lauryl sulfate, alcohol, harsh scrubbing
2. Treatment Active (Optional)
If you’re using morning actives like azelaic acid or niacinamide, apply to clean, dry skin.
Wait time: 1-2 minutes before next step
3. Antioxidant Serum
Vitamin C serums protect against environmental damage and help with both acne scarring and aging.
Best for acne-prone skin: L-ascorbic acid formulations in lightweight, non-greasy bases
4. Moisturizer
Yes, even acne-prone skin needs moisture—especially during menopause.
What to look for: Lightweight, non-comedogenic, containing hyaluronic acid, ceramides, or peptides
Avoid: Heavy oils, thick butters, pore-clogging ingredients
5. SPF (Non-Negotiable)
This is absolutely critical, especially if you’re using retinoids or other active ingredients.
Minimum: SPF 30, broad spectrum
For acne-prone skin: Mineral sunscreens (zinc oxide, titanium dioxide) or lightweight chemical formulas labeled non-comedogenic
Evening Routine
1. Double Cleanse
First cleanse: Remove makeup and SPF with an oil cleanser, micellar water, or cleansing balm
Second cleanse: Use your regular gentle cleanser
2. Treatment Actives
This is when you use your retinoid (the most important product for both acne and aging).
How to apply: Pea-sized amount to clean, completely dry skin
Buffer method: If your skin is sensitive, apply moisturizer first, wait 20 minutes, then apply retinoid
3. Spot Treatments
Apply benzoyl peroxide or salicylic acid only to active breakouts, not all over.
4. Hydration Layer
Hyaluronic acid serum applied to slightly damp skin, or peptide serums for anti-aging benefits.
5. Moisturizer
Evening moisturizer can be richer than morning but should still be non-comedogenic.
Look for: Ceramides, niacinamide, peptides, squalane
What to AVOID
- Harsh physical scrubs: Scrubbing doesn’t clear acne and can worsen inflammation
- Alcohol-heavy toners: Stripping your skin triggers more oil production
- Over-cleansing: Washing more than twice daily damages your barrier
- Too many actives at once: Introduce one new product every 2-3 weeks
- Picking and popping: Mature skin scars more easily
- Heavy, pore-clogging oils: Coconut oil, cocoa butter (some lighter oils are fine)
Ingredients That Work for Both Acne and Aging
- Retinoids/retinol (the MVP)
- Niacinamide
- Azelaic acid
- Peptides
- Ceramides
- Hyaluronic acid
- Vitamin C
- Alpha hydroxy acids (glycolic, lactic) in low concentrations
Product Selection Reality Check:
- “Non-comedogenic” labels aren’t regulated but are still a helpful guide
- Patch test new products on your jawline for a week
- Introduce only one new product at a time
- Give products 6-8 weeks to work before deciding they’re not effective
- Simpler routines are often more effective than complicated ones
Professional Treatments and In-Office Options
Sometimes at-home care needs backup from the professionals.
Chemical Peels
Professional-strength salicylic acid or glycolic acid peels can help unclog pores, reduce inflammation, and improve texture and fine lines simultaneously.
Frequency: Every 4-6 weeks
Cost: $100-300 per treatment
Downtime: Minimal to moderate peeling for 3-7 days
Laser and Light Therapies
- Blue light therapy: Kills acne-causing bacteria
- IPL (Intense Pulsed Light): Reduces inflammation, redness, and can improve sun damage
- Laser for scarring: Fraxel or CO2 lasers help with acne scarring (once active acne is controlled)
Cost: $200-600+ per session
Sessions needed: Usually multiple (4-6 for acne, more for scarring)
Professional Extractions
When done properly by an esthetician or dermatologist, extractions can safely remove stubborn comedones without causing scarring.
Never DIY: Deep cystic acne should never be squeezed or picked—you’ll make it worse and risk scarring
Cortisone Injections
For deep, painful cystic breakouts, a dermatologist can inject diluted cortisone directly into the lesion.
Results: Dramatic improvement in 24-48 hours
Cost: Usually covered by insurance as a medical procedure
When to ask: Before important events or when you have particularly painful cysts
HydraFacial and Medical-Grade Facials
These provide deep cleaning and light exfoliation without irritation, good for ongoing maintenance.
Frequency: Monthly
Cost: $150-300
When to See a Dermatologist
Don’t suffer in silence. Here’s when it’s time to get professional help.
Red Flags That Require Medical Attention
- Sudden, severe acne with no previous history
- Acne not responding to 3 months of consistent OTC treatment
- Deep, painful cystic acne
- Acne causing scarring or significant post-inflammatory hyperpigmentation
- Breakouts accompanied by other symptoms:
- Excessive facial hair growth (hirsutism)
- Rapid, unexplained weight gain
- Thinning hair on your scalp while body hair increases
- Severe mood changes beyond typical menopause symptoms
- Extreme fatigue
These could indicate other hormonal conditions like PCOS, thyroid disorders, or adrenal issues that need medical evaluation.
What to Expect at Your Appointment
Your dermatologist will:
- Review your medical and menstrual history
- Examine your skin and breakout patterns
- Possibly order hormone level testing (testosterone, DHEA-S, sometimes others)
- Discuss your symptoms and timeline
- Create a personalized treatment plan
- Prescribe medications if appropriate
How to Prepare
- Track your symptoms: Note when breakouts occur, where, potential triggers
- List products tried: Bring a list of what you’ve used and for how long
- Document other menopause symptoms: This helps connect the dots
- List all medications and supplements: Some can affect acne or interact with treatments
- Come with a bare face: No makeup so your skin can be properly examined
Finding the Right Provider
Dermatologist: Best for prescription treatments, in-office procedures, and complex cases
Gynecologist/Menopause specialist: Can address hormonal causes, prescribe HRT, coordinate care
Combination approach: Often ideal to have both dermatology and hormone management
Telemedicine options: Many dermatologists now offer virtual consultations, which can be more convenient and affordable
Advocating for Yourself
If a healthcare provider dismisses your concerns, find another one. You deserve to:
- Be taken seriously regardless of age
- Have access to effective treatments
- Get answers about why you’re suddenly breaking out
- Feel comfortable in your skin
The mental health impact of adult acne is real and valid. Seeking treatment isn’t vanity—it’s self-care.
Long-Term Management and Realistic Expectations
Let’s talk about what success actually looks like with menopausal acne treatment.
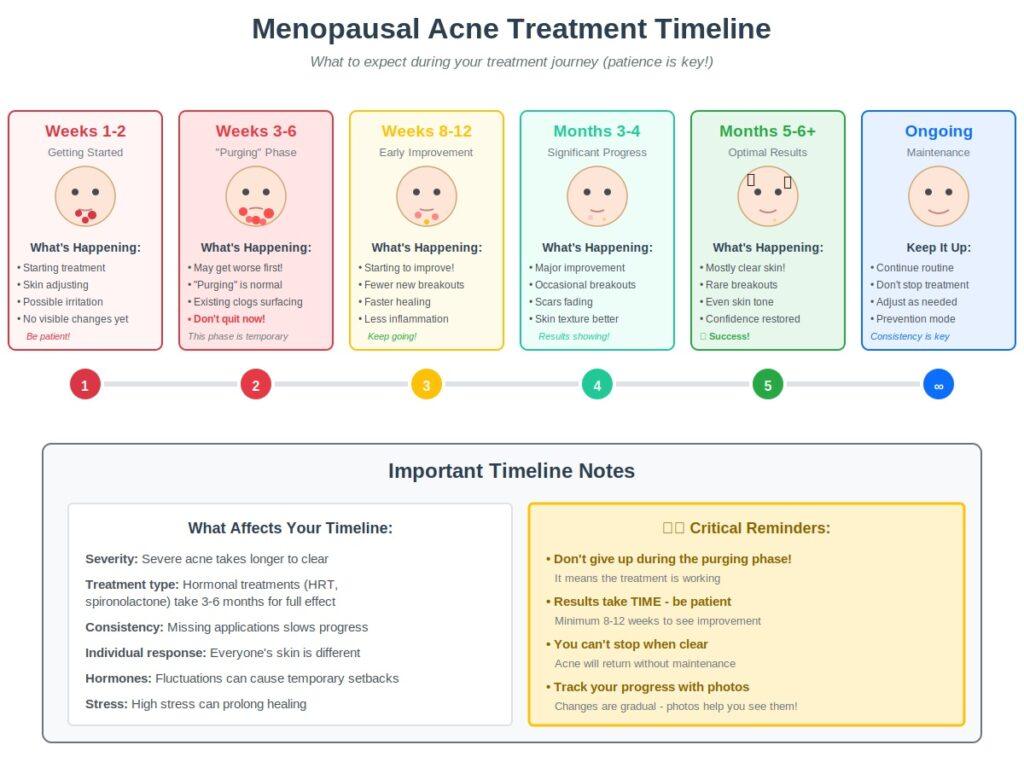
The Treatment Timeline: What to Expect
Weeks 1-4: You’re getting started. You might see purging if using retinoids. Stick with it.
Weeks 6-8: Starting to see some improvement. Fewer new breakouts, existing ones healing faster.
Months 3-4: Significant improvement. Breakouts are less frequent, less severe, and heal more quickly.
Months 6+: Optimal results with most treatments. Skin is clearer, texture is better, scarring is fading.
The reality: Progress isn’t linear. You’ll have setbacks, especially around stress, dietary changes, or if you’re still experiencing hormonal fluctuations.
Maintenance is Key
Here’s the truth: with hormonal acne, you can’t just stop treatment once you’re clear. The underlying hormonal imbalance doesn’t go away on its own (unless you address it with HRT or wait for post-menopause stabilization).
Successful long-term management means:
- Continuing your skincare routine even when clear
- Staying on oral medications as prescribed (you can often reduce doses over time)
- Adjusting your routine as your skin changes seasonally or with age
- Being proactive rather than reactive
Managing Expectations
What “clear” looks like: Occasional breakouts are still normal. Clear skin doesn’t mean perfect skin 365 days a year—it means manageable, infrequent breakouts that don’t significantly impact your life.
Combination approaches work best: Most women find that using multiple treatments (topical + oral, or HRT + topical) provides better results than any single treatment.
Individual response varies: What works amazingly for your friend might not work for you. Be patient and willing to adjust.
Lifestyle Factors That Help
While you can’t lifestyle your way out of hormonal acne, these factors make a difference:
Stress Management:
Chronic stress elevates cortisol, which worsens hormonal acne. Practices that actually help: regular exercise, meditation, adequate sleep, therapy, setting boundaries.
Sleep Quality:
Poor sleep disrupts hormone regulation and increases inflammation. Aim for 7-9 hours of quality sleep.
Diet Considerations:
The research isn’t definitive, but many women notice connections:
- Dairy: May worsen acne for some (hormones in milk)
- High glycemic foods: Sugar and refined carbs can trigger insulin spikes that worsen acne
- Anti-inflammatory diet: Mediterranean-style eating may help reduce overall inflammation
Supplements that might help:
- Omega-3 fatty acids (anti-inflammatory)
- Zinc (if deficient)
- Vitamin D (if levels are low)
- Probiotics (emerging research on gut-skin connection)
Exercise:
Regular movement helps regulate hormones and reduce stress. Just make sure to cleanse your face promptly after sweating.
Hydration:
Adequate water intake supports skin health and function.
The Emotional Component
Let’s acknowledge the mental health impact of dealing with acne in your 40s, 50s, or beyond.
It’s frustrating. It’s embarrassing. It feels unfair. You’re dealing with wrinkles and breakouts simultaneously—it’s like the worst of both worlds.
This is not vanity—it’s quality of life. Research shows that adult acne significantly impacts mental health, self-esteem, and even career confidence.
Finding support helps:
- Online communities of women dealing with the same thing
- Therapy if acne is significantly affecting your mental health
- Being open with friends and family
- Remembering you’re not alone—millions of women go through this
The Silver Lining
Here’s some hope: most women see improvement 2-5 years after their final menstrual period, once hormones stabilize at their new post-menopausal baseline.
Also, treatment options are better now than ever before. We understand the hormonal mechanisms better, we have more targeted treatments, and dermatologists are increasingly trained in managing adult, hormonal acne.
You don’t have to just accept this as your new normal. Effective treatments exist, and you deserve to feel comfortable in your skin.
Frequently Asked Questions
Q: How long does menopausal acne last?
A: Menopausal acne typically starts during perimenopause (40s) and can continue through the menopausal transition and early post-menopause. Most women see natural improvement 2-5 years after menopause once hormones stabilize at their new baseline. However, with appropriate treatment, symptoms can be significantly reduced much sooner—often within 3-6 months.
Q: Can you get acne for the first time during menopause?
A: Absolutely yes. About 25% of women experience acne for the first time in their 40s or 50s, even if they had perfectly clear skin as teenagers. This is entirely due to the changing hormone ratios as estrogen declines relative to androgens.
Q: Will HRT cure my menopausal acne?
A: HRT can significantly improve menopausal acne by restoring estrogen levels and rebalancing the estrogen-androgen ratio. However, it’s not an instant cure, and some women still need additional topical or oral treatments even while on HRT. The type of progestin in your HRT formulation matters significantly—anti-androgenic progestins help while others may worsen acne. Improvement typically takes 3-6 months.
Q: Is menopausal acne painful?
A: Yes, menopausal acne is often significantly more painful than teenage acne because it tends to be deeper, cystic acne rather than surface breakouts. These deep lesions create inflammation far below the skin’s surface, making them tender to the touch. The pain can last for weeks as the breakout slowly resolves.
Q: What’s the best treatment for menopausal acne?
A: A combination approach typically works best. Addressing the hormonal root cause (with HRT, spironolactone, or anti-androgenic birth control for those still cycling) plus topical treatments (particularly retinoids) gives most women the best results. The specific best treatment varies by individual, so working with a dermatologist for a personalized plan is ideal.
Q: Can diet affect menopausal acne?
A: While diet isn’t the primary cause of hormonal acne, it can be a contributing factor. Some women find that reducing dairy products, limiting high-glycemic foods (sugar, refined carbs), and following an anti-inflammatory diet helps improve their acne. The gut-skin connection is an emerging area of research. That said, diet changes alone rarely clear hormonal acne—they work best as part of a comprehensive treatment plan.
Q: Is menopausal acne worse than teenage acne?
A: It’s different rather than necessarily worse. Menopausal acne tends to be deeper, more painful, and slower to heal than teenage acne. It also carries a higher risk of scarring. However, it typically affects a smaller area (mainly the lower face and jawline) rather than the entire face. Many women find it more psychologically distressing because it’s unexpected and occurs during a life stage when they thought they were done with acne.
Q: Do retinoids help with both acne and wrinkles?
A: Yes! Retinoids (prescription) and retinol (OTC) are the gold standard for both acne treatment and anti-aging skincare. They work by increasing cell turnover, which unclogs pores and prevents breakouts while simultaneously improving fine lines, skin texture, and boosting collagen production. This makes them ideal for treating menopausal acne since they address both concerns at once.
Q: Why is my skin dry and breaking out at the same time?
A: This is one of the most frustrating aspects of menopausal acne. As estrogen declines, your skin produces less natural moisture and your barrier function weakens—leading to dryness. At the same time, the relative increase in androgen activity triggers excess sebum production in specific areas. You end up with skin that’s simultaneously dry (overall) and oily (in the breakout zones). This requires a balanced approach: gentle, hydrating products that don’t strip your skin, combined with targeted acne treatments only where needed.
Conclusion
If you’re dealing with menopausal acne, first know this: it’s completely normal, incredibly common, and most importantly—treatable. You’re not imagining it, you’re not doing anything wrong, and you’re definitely not alone.
While menopausal acne looks and behaves differently than teenage breakouts—appearing primarily on your jawline and chin as deep, painful lesions—the silver lining is that we now understand the hormonal mechanisms driving it and have multiple effective treatment options.
Whether you choose to address the hormonal root cause with HRT or spironolactone, use targeted topical treatments like retinoids and azelaic acid, or combine multiple approaches, clear skin is achievable. It requires patience (results take months, not days), consistency, and often guidance from a dermatologist who takes your concerns seriously.
You deserve to feel comfortable in your skin at every age. Seeking treatment for menopausal acne isn’t vanity—it’s self-care and a quality of life issue. Don’t let anyone, including healthcare providers, dismiss your concerns because you’re “too old” for acne treatment.
Your skin is going through a major transition, and with the right approach, you can navigate it successfully. Be patient with yourself, be willing to try different treatments to find what works for you, and remember that even after menopause, when hormones stabilize, most women see natural improvement.
In the meantime, you have options, support, and an entire community of women going through the same experience. You’ve got this.
Learn More
- Perimenopause Symptoms: The Complete Guide to 50+ Signs Your Body is Changing
- Best Lotion for Menopausal Dry Skin: What Actually Works (Body & Face)
- The Truth About Menopause Hormone Balance: An Expert Guide for Women Over 45
This article is for informational and educational purposes only and does not constitute medical advice. The content provided is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition or treatment.